
Primary Tuberculosis of the Appendix
Leo F. Tauro, P. Sathyamoorthy Aithala, SR Celine George, Hanumanthappa, John Martis
doi:10.5001/omj.2010.72
ABSTRACT
Primary (isolated) tuberculosis of the appendix is a clinical rarity, its reported incidence being 0.1 to 0.3%. Diagnosis is often made only after histopathological examination of resected specimen. This report describes two patients with clinical diagnosis of acute appendicitis and appendicular mass respectively, who were finally diagnosed to have tuberculosis of the appendix on histopathological examination. This article stresses the importance of histopathological examination of resected appendix.
From the Department of Surgery, Fr. Muller Medical College Hospital, Muller Road, Kankanady Post, Mangalore, South Kanara 575002, India.
Received: 07 May 2010
Accepted: 12 June 2010
Address correspondence and reprint request to: Dr. Leo F. Tauro, Department of Surgery, Fr. Muller Medical College Hospital, Muller Road, Kankanady Post, Mangalore, South Kanara 575002, India.
E-mail: drlftauro@rediffmail.com
INTRODUCTION
The prevalence of isolated appendicular tuberculosis in all appendicectomies performed varies from 0.1 to 3.0% cases.1-3 Its incidence among the patients who are known cases of tuberculosis is 1.5 to 30%.3-6 Primary (isolated) tuberculosis of the appendix is a clinical rarity.6 We report two cases of primary (isolated) tuberculosis of appendix with no detectable tuberculosis focus elsewhere in the body.
CASE REPORT
Case 1
A 28 year-old male was admitted with severe abdominal pain in the right iliac fossa along with fever and vomiting for four days. On examination, the patient was well built and well nourished. Examination of his respiratory and cardiovascular systems was normal. Abdominal examination revealed tenderness and rebound tenderness in the right iliac fossa without any palpable mass. His routine hematological and urine examination were normal except for leukocytosis and neutrophilia. Sputum examination for AFB was negative. Chest X-ray showed no abnormality and abdominal ultrasonography revealed inflamed appendix.
With the diagnosis of acute appendicitis, the patient was subjected to appendicectomy through Lanz incision. On peritoneal cavity exploration, the appendix was found thickened, inflammed with minimal adhesions in the peri-appendicular tissues. No palpable pathology was detected in the ileum, caecum and mesentery. Mesenteric lymph nodes were not enlarged. Appendicectomy was performed and the specimen was subjected to histopathological examination.
Gross examination of the specimen revealed appendix and periappendicular fibro fatty tissue measuring about 7 cm in length with grayish white appearance. Cut surface showed the narrowed lumen of the appendix with thickened wall.
No mucosal ulceration was seen, however, microscopic examination revealed tuberculous granulomas in the mucosa, sub mucosa and muscle layers of the appendix consisting of epitheloid cells, Langhan’s giant cells, lymphocytes, mononuclear cells and central area of caseous necrosis. (Figs. 1 & 2)
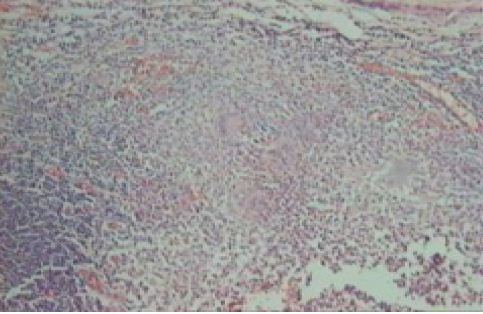
Figure 1: Photomicrograph of appendix showing tubercular granuloma (low power).

Figure 2: Tubercular granuloma under high power.
Periappendicular tissue did not show any tubercular lesion. Antitubercular treatment (ATT) was started with four drugs in conventional doses, as the diagnosis was tuberculous appendicitis.
The patient had an uneventful postoperative recovery. He successfully completed nine months’ ATT with complete final recovery. After one year follow up, he remains asymptomatic.
Case 2
An 18 year-old female patient was admitted with abdominal pain, fever and vomiting for five days. On examination, the patient had an average built and was poorly nourished. Examination of cardiovascular and respiratory system was normal. Abdominal examination revealed a tender, firm, ill-defined and fixed mass 6x5 cm size in the right iliac fossa. Bowel sounds were normal. Her routine hematological examination revealed leukocytosis and neutrophilia. Urine examination was normal, sputum AFB was negative, and chest X-ray was normal. Abdominal Ultrasonography revealed a mass of size 5x7 cm comprising of bowel and omentum in the right iliac fossa without any collection.
The patient was treated conservatively with parental antibiotics and was discharged on oral antibiotics for two weeks. On follow up, the mass had resolved. She was subjected to interval appendicectomy after six weeks. Intra-operative and histopathological examination findings were similar to the first case which revealed tubercular appendicitis. She had an uneventful postoperative recovery and successfully completed nine month’s ATT with complete recovery. After two years follow up, the patient remains asymptomatic.
DISCUSSION
The incidence of primary tuberculosis of the appendix in appendicectomies performed varies from 0.1 to 3.0%.1,2,3 Technically, such a diagnosis can only be made after histopathological examination. Secondary involvement of the appendix from ileocaecal tuberculosis is also uncommon and varies from 1.5 to 3%.1-3 Autopsy figures among patients of tuberculosis also reveal appendicular involvement in about 30% of cases. Most of the literature regarding tuberculous appendicitis pertains to pre-chemotherapeutic era and the disease is seldom reported nowadays. We came across only two cases of tuberculous appendicitis over a period of eight years.
The rarity of primary tuberculosis of the appendix may be due to the fact that there is minimal contact of appendicular mucosa with intestinal contents.1-3 Though gastrointestinal tuberculosis is mostly secondary to pulmonary disease, the route of infection is by swallowing i.e. intraluminal.3,4 The open cases of pulmonary tuberculosis in our country are likely to contaminate food and
ther objects, the use of which may lead to primary intestinal tuberculosis in people who have unhealthy habits.3 This was the probable mode of infection in the reported cases.
Three clinical types of tuberculous appendicitis have been described in literature.3,7 The first type presents as an acute form indistinguishable from pyogenic appendicitis until histologically proven. The second clinical type is a chronic form presenting with vague pain, occasional history of vomiting, diarrhoea and a mass in the right iliac fossa. These cases are indistinguishable from cases of ileocaecal tuberculosis. The third type is a latent one found accidentally on histopathological examination.
CONCLUSION
Primary (isolated) tuberculosis of appendix may or may not be associated with specific clinical features, and diagnosis is often made only after histopathological examination. Therefore, it is strongly recommended that all appendicectomy specimens should be subjected to histopathological examination to exclude tuberculosis and other pathology.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding was received on this work.
-
Braasted FW, Dockerty MB, Waugh JM. Tuberculosis appendicitis. Surgery 1950,27(5):790
-
Sinh MK, Arunabh, Kapoor VK. Tuberculosis of the appendix – a report of 17 cases and a suggested etiopathological classification. Post grad Med J 1987; 63:855-7.
-
Nuwal PI, Dixit R, Jain S, Porwal V. Isolated Appendicular Tuberculosis – A case report, Ind. J. Tub 2000, 47:241-2
-
Shah RC, Mehta KN, Jahindhwala JM, Tuberculosis of appendix. J. Ind Med Assoc 1967, 49(3):138-40
-
Mittal VK, Khanna SK, Gupta NM, Aikat M. Isolated Tuberculosis of appendix. Am. Surg. 1975 Mar, 41(3) : 172-4
-
Shalaby AMR. Tuberculous appendicitis. Inter J of Path 2007; 6(2).
-
Bobrow ML, Friedman S. Tuberculosis appendicitis. Am J. Surg 1956, 91:389.
How to cite this URL
Tauro LF, Aithala S, George SRC, Hanumanthappa, Martis J. Primary Tuberculosis of the Appendix. OMJ [Online] 2010 July; 25(3). Available at http://www.omjournal.org/CaseReports/FullText/201007/FT_7PrimaryTuberculosisoftheAppendix.html.