
A Rare Case of Laryngocele in a Young Omani Male
Binu R. George,1 Suhel Hasan,1 Naveen Kumar G,1 Salem MS. Tobook,1 Manjula Dhinakar 2
George BR, et al. OMJ. 25, (2010); doi:10.5001/omj.2010.45
ABSTRACT
Laryngocele is a cystic dilatation of the laryngeal saccule. The saccule presents as a diverticulum from the anterior end of the ventricle and extends upwards between the vestibular fold and the inner aspect of the thyroid cartilage. Factors that increase intra laryngeal pressure can lead to the development of laryngocele. Laryngocele mainly affects males in the sixth decade and is usually unilateral. This is a report of a rare case laryngocele in a young Omani male patient.
From 1ENT Department, Sultan Qaboos Hospital, Salalah, Sultanate of Oman 2Department of Radiology, Sultan Qaboos Hospital, Salalah, Sultanate of Oman.
Received: 21 Jan 2010
Accepted: 13 Feb 2010
Address correspondence and reprint request to: Dr. Binu R. George, Specialist, ENT Dept.Sultan Qaboos Hospital, Salalah, Sultanate of Oman.
Email: trc_binurg@hotmail.com
George BR, et al. OMJ. 25, (2010); doi:10.5001/omj.2010.45
INTRODUCTION
Laryngocele is a cystic dilatation of the laryngeal saccule. It may be internal or External. The usual presentation is a swelling in the upper neck and the diagnosis is confirmed radiologically with the help of X-rays and Computed Tomograghy Scans. Connection between the air sac and the airway helps to establish the diagnosis. Surgery is indicated for symptomatic Laryngoceles and for cosmetic reasons.
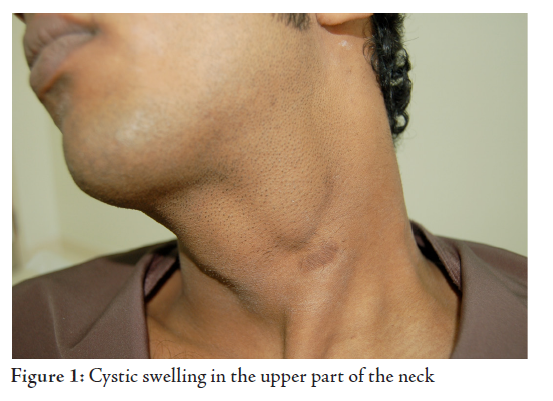
A 23 year old male patient, non smoker, shop keeper by profession presented to the Ear Nose Throat Out Patient Department with complaints of painless swelling in the upper part of the left side of neck. The patient did not have a cough, change of voice , difficulty in swallowing or difficulty in breathing. The patient had a history of surgery in the neck eight years ago for similar complaints, following which he was symptom free. The swelling reappeared after six years and has gradually increased in size over the past two years.
On examination the patient had a diffuse, non tender, cystic swelling in the upper part of the neck on the left side. The swelling was approximately 4cm x 3cm in size and extended below the lower border of the mandible to the level of the lower border of the thyroid cartilage in the anterior triangle, (Fig. 1). The swelling was compressible and increased in size when the patient performed the Valsalva manoeuvre and on coughing. The skin below the swelling showed the scar from the previous surgery.
Fiber optic Laryngoscopy revealed a mild bulge at the level of the left false cord. The rest of the larynx and vocal cords were normal. Antero posterior soft tissue neck X-ray showed a large air filled sac in the left side of the neck, (Fig. 2). The sac was shown to be connected to the airway by a small stalk. The internal component on the right side could also be clearly visualized.

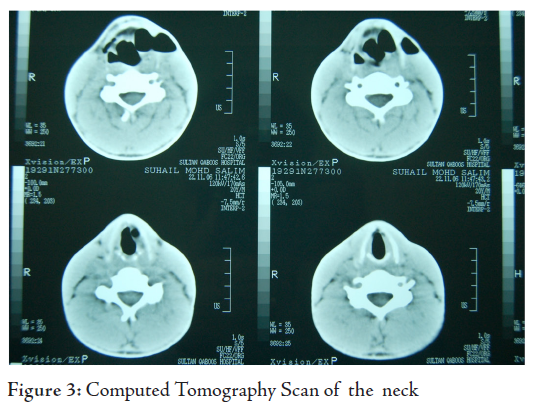
Computed Tomography Scan of the neck showed the presence of the Laryngocele as a well defined, smooth, air filled sac in the superior paralaryngeal space, (Fig. 3). The connection between the air sac and the airway helped to establish the diagnosis. The patient had a mixed Laryngocele on both sides with a large extralaryngeal component on the left side and a small extralaryngeal componenton the right side
After the diagnosis was confirmed, the patient was taken for surgical excision of the laryngocele for cosmetic reasons. Excision was performed under general anaesthesia. The lesion was approached via a skin crease incision over the swelling.
Subplatysmal skin flaps were developed and the fundus of the laryngocele was freed by a sharp dissection, (Figs. 4,5).

The neck of the laryngocele was followed down through the thyrohyoid membrane. Special care was taken to avoid injury to the Superior Laryngeal Nerve. Upon reaching the laryngeal mucosa, the neck of the laryngocele was ligated and divided. The small laryngocele on the opposite side was not excised as the patient did not have any symptoms on the right side. The wound was then closed in layers.
The post operative period was uneventful and sutures were removed on the seventh post operative day. The patient has been on follow up at the OPD after surgery. The patient was asymptomatic with no recurrence of the swelling.
DISCUSSION
Laryngocele has a male to female ratio of 5:1 with peak incidence in the sixth decade.
Three types of laryngocele have been described.
1. Internal: When the laryngocele is confined to the interior of the larynx and extends posterosuperiorly into the false cord and the ary epiglottic fold. It appears on laryngoscopy as a smooth swelling in the supraglottis.
2 . Externa: When the laryngocele extends superiorly and appears laterally in the neck through an opening in the Thyrohyoid membrane. It clinically presents as a swelling in the neck at the level of the hyoid bone anterior to the Sternomastoid muscle.
3. Combined: When there is simultaneous existence of both features.1-4
The laryngocele is bilateral in one third of cases.1 Congenitally, the laryngeal saccule is remnant corresponding to the lateral laryngeal air sacs of the higher anthropoid apes which may on occasion be manifest suddenly in response to increase in intralaryngeal pressure. An acquired laryngocele may develop due to any factor which increases the intra glottic pressure such as coughing, straining, playing wind instruments or glass blowing.1,2,5 Another aetiology may be air trapping due to ball valve closure of the neck of the saccule, allowing the entry of air into the saccule, but preventing its Egress.5 This can occur from inflammatory or neoplastic process in the ventricle or false cord. The incidence of laryngocele in patients with laryngeal cancer has been estimated to be around 10% (ranging from 4.9 - 54%) and so it is important to rule out malignancy in all patients with laryngocele.6
Most patients are asymptomatic. Patients with external laryngocele may present with a swelling on one or both sides of the neck. The swelling is usually compressible and increases in size on perfirming the Valsalva manoeuvre. Other patients may present with cough, change of voice, stridor or sore throat. Hence, others may present with major complications such as pyocele or acute airway obstruction. The diagnosis can be reached using any of the following modalities:
1. Fibre optic laryngoscopy shows a smooth swelling in the supraglottis, usually at the level of the false cord.
2. Soft tissue neck X-ray shows a well defined, round or oval radiolucent area in the paralaryngeal soft tissues. Films taken in the antero posterior position are more useful than lateral films in outlining the laryngocele. In the lateral position, a small laryngocele may be superimposed on the normal laryngeal shadow and may be overlooked.
3. Computerised Tomography scan shows a well defined, smooth, air filled sac in the lateral aspect of the superior paralaryngeal space. The connection between the air sac and the airway helps to establish the diagnosis. CT scan provides a non invasive and effective radiological investigation of the larynx. It can be performed with minimal risks even in the presence of respiratory obstruction and shows the laryngeal cartilages and structures at the glottis level well.
4. Magnetic Resonance Imaging. Nowadays, MRI has become the investigation tool of choice in showing the laryngocele because of its better superior soft tissue resolution.
The differential diagnosis mainly includes any cystic swelling in the upper part of the neck like branchial cyst, submandibular salivary gland duct cyst, cystic hygroma, saccular cyst, mucous retention cyst, thyroglossal duct cyst and neck swellings which increase in size on valsalva manoeuvre like Jugular vein phlebectasia. A saccular cyst should also be kept in mind when an internal layngocele is diagnosed. A pharyngocele also presents as a cystic swelling in the upper part of the neck.
Asymptomatic lesions found incidentally can be managed conservatively. Absolute indications for excision include symptomatic combined laryngocele and suspicion of malignancy.5 Cosmetic concern is a relative indication for excision. Excision can either be through an endoscopic approach using a CO2 laser for internal laryngocele or via an external approach for external laryngoceles. The external cervical approach allows good exposure of the lesion with minimal functional disability. Removal of a triangular wedge of thyroid lamina provides wide exposure to the paraglottic space, thus helping in the internal dissection of the laryngocele.5
CONCLUSIONThe diagnosis of Laryngocele should be kept in mind in cases of upper neck swelling. Radiological investigations such as Soft tissue neck and CT Scans help to confirm the diagnosis. Direct Laryngoscopy is essential to rule out malignancy before surgical excision of the laryngocele.
The authors reported no conflict of interest and no funding was received on this work.
-
Stell PM , Maran AG. Laryngocele. J Laryngol Otol 1975;89 (9):915-924.
-
Amin M, Maran AG. The aetiology of Laryngocele. Clin Otolayngol Allied Sci 1988; 13(4):267-272.
-
Nazaroglu H, Ozates M, Uyar A, Deger E, Simsek M. Laryngopyocele- Signs on Computed Tomography Eur J Radiol 2000; 33(1):63-65.
-
Rutka J, Birt D Laryngocele: a case report and review J Otolaryngol 1983; 12(6):389-392.
-
Rosen CA, Simpson CB. Operative Techniques in Laryngology. 1st Edition. Berlin Heidelberg, Springer-Verlag, 2008.
-
Close GL, Merkel M, Deaton WC, Burns DK, Schaffer SD. A Symptomatic Laryngocele: incidence and association with laryngeal cancer. Ann Otol Rhinol Laryngol 1987; 96:393-399.