
Hemosuccus Pancreaticus: A Rare Cause Of Upper Gastrointestinal Bleeding During Pregnancy
Rani Akhil Bhat,1 Vani Ramkumar,1 K. Akhil Krishnanand Bhat, 2 Rajgopal Shenoy2
Bhat RA, et al. OMJ. 25 (2010); doi:10.5001/omj.2010.21
ABSTRACT
Upper gastrointestinal bleeding is most commonly caused by lesions in the esophagus, stomach or duodenum. Bleeding which originates from the pancreatic duct is known as hemosuccus pancreaticus. Only a few scattered case reports of hemosuccus pancreaticus during pregnancy have been recorded in literature. This is a case of a primigravida with 37 weeks of gestation with hemosuccus pancreaticus and silent chronic pancreatitis. Evaluating pregnant women with upper gastrointestinal bleeding differs from that of non pregnant women as diagnostic modalities using radiation cannot be used. Therefore, Esophagogastroduodenoscopy should be performed at the time of active bleeding to diagnose hemosuccus pancreaticus.
From the 1Department of Department of Obstetrics and Gynaecology, Oman Medical College, Sohar, Sultanate of Oman, 2Department of Surgery, Oman Medical College, Sohar, Sultanate of Oman.
Received: 06 Nov 2009
Accepted: 31 Dec 2009
Address correspondence and reprint request to: Dr. Rani A. Bhat,Department of Obstetrics and Gynaecology, Oman Medical College, P. O. Box 391, P. C. 321, Al-Tareef, Sohar, Sultanate of Oman. E-mail: drraniakhil@hotmail.com
INTRODUCTION
Hemosuccus pancreaticus is the term used to describe the syndrome of gastrointestinal bleeding into the pancreatic duct manifested by blood loss through the ampulla of Vater. It is the least frequent cause of upper gastrointestinal bleeding (1/1500) and is observed predominantly in men (sex ratio 7:1). 1 It is most often caused by chronic pancreatitis, pancreatic pseudocysts, and pancreatic tumors. Bleeding occurs when a pseudocyst or tumor erodes into a vessel, forming a direct communication between the pancreatic duct and the blood vessel. Hemosuccus pancreaticus is often difficult to diagnose, partly because of its rarity and due to its anatomical location. Also, because the bleeding is often intermittent and cannot be easily diagnosed by esophagogastroduodenoscopy in the intermittent phase. This case report describes a pregnant woman with hemosuccus pancreaticus and silent chronic pancreatitis.
CASE REPORT
A 33 year old primigravida with 37 completed weeks of gestation was admitted to Oman Medical College hospital with recurrent episodes of melena and hematemesis. There was no other positive medical or surgical history. On physical examination, the patient was pale, blood pressure was 100/60 mm of Hg and pulse rate was 110 beats/min. On abdominal examination, the height of the uterus was corresponding to 34 weeks of gestation and with a breech presentation. Ultrasound of the fetus showed a single fetus of 34 weeks with asymmetrical intrauterine growth restriction (IUGR) with AFI of 7 and normal Doppler study. Rectal examination showed a combination of dark red blood and melena. Laboratory investigations revealed hemoglobin of 6.3 grams/dL, liver function tests, serum amylase, glucose and prothrombin time were within the normal range. Ultrasound of the abdomen revealed no pathology. Esophagogastroduodenoscopy and colonoscopy performed to investigate hematemesis and melena were normal. In view of fetal growth restriction, breech presentation and critical condition of the mother, she had a elective cesarean section and delivered a live 2 kg male baby. Abdominal exploration at the time of cesarean section revealed a hard pancreas with woody feeling of the gland throughout. Repeat endoscopy performed following a short period of hematemesis showed bleeding from ampulla of Vater, hence the diagnosis of hemosuccus pancreaticus was made, (Fig. 1). Computed tomography scan following delivery showed calcification of pancreas suggestive of chronic pancreatitis. She was referred to higher center for further management where she underwent pancreaticoduodenectomy. The patient was being treated for chronic pancreatitis and was followed up for almost two years since admission, the bleeding did not reccur.
DISCUSSION
Hemosuccus pancreaticus is a very rare cause of upper gastrointestinal bleeding. Approxiamtely 100 cases have been reported in the literature since it was first reported by Lower in 1931. 2 In 80% of the cases, hemosuccus pancreaticus complicates an underlying pancreatic disease; 20% of the cases correspond to a vascular anomaly.3 Since there has been no case reported, it is unclear if pregnancy precipitates this condition in women with underlying chronic pancreatitis. The patient presented with typical
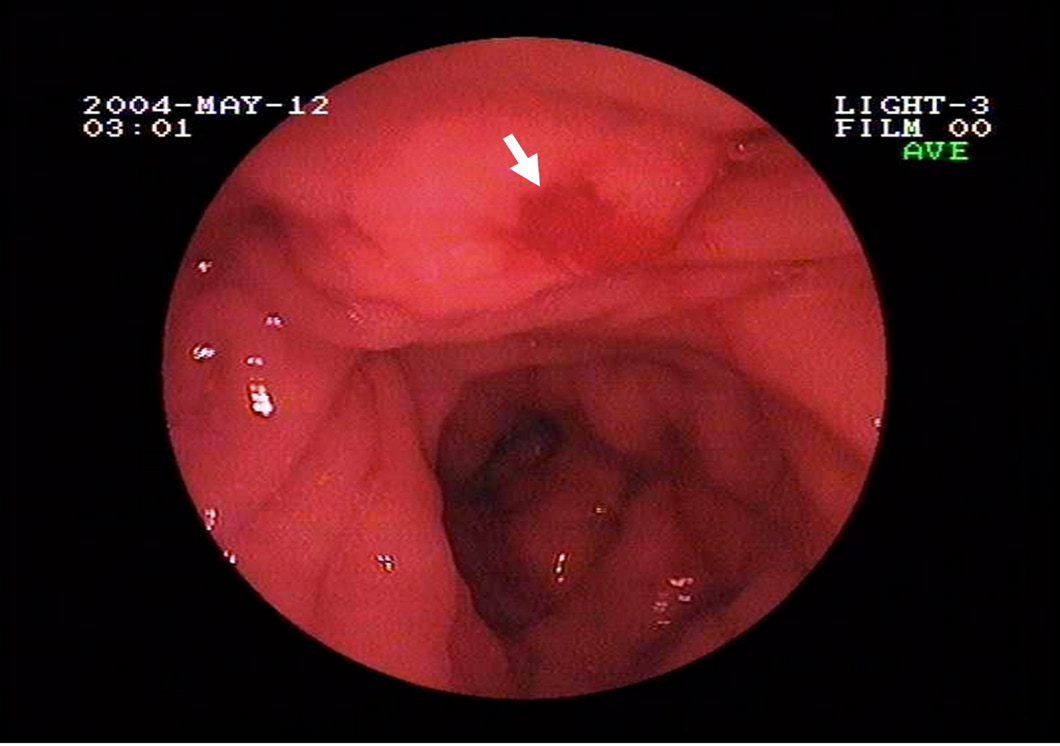
Figure 1: Endoscopic picture showing bleeding from ampulla of Vater.
features of abdominal pain and intermittent gastrointestinal bleeding. The intermittent nature of the bleeding is very specific and is due to clot formation in the main pancreatic duct.2
Endoscopy is essential to rule out other causes of upper gastrointestinal bleeding and in rare cases, active bleeding can be seen from the duodenal ampulla. Diagnosis in this patient was delayed as the initial endoscopy was normal and the patient did not have any other features of chronic pancreatitis. Late diagnosis is however common due to the intermittent nature of the bleeding.2
Hence, endoscopic procedure needs to be repeated as it can be normal in the event of intermittent bleeding. Other investigations such as ultrasonography, duplex scan, endoscopic retrograde cholangiopancreatography, selective arteriography, computed tomography (CT) and angio-CT can give information on the type of pancreatic pathology.4 Evaluating pregnant women differs from non-pregnant women as the gravid uterus may hamper visualization of the pancreas on ultrasonography and radiation technologies cannot be widely used during pregnancy due to radiation exposure to the fetus. If indicated, endoscopic procedures can be performed with additional safety precautions to minimise the duration of the procedure and radiation exposure to the fetus.5
Esophagogastroduodenoscopy should be considered as the gold standard test to evaluate pregnant women with upper gastrointestinal bleeding. Management of hemosuccus pancreaticus during pregnancy requires a multidisciplinary approach and should be individualized according to the period of gestation, fetal lung maturity and severity of the disease.
When hemosuccus pancreaticus occurs in patients without
pseudoaneurysms or pseudocysts, it can be treated conservatively with modalities
such as arterial embolization.6 Surgery, in the form of
pancreaticoduodenectomy is required when embolization fails or is unavailable,
when there is recurrence of bleeding after embolization, when bleeding is
associated with pseudoaneurysms of peripancreatic arteries or pseudocysts, or in
case of hemodynamic instability.7,8
CONCLUSION
Hemosuccus pancreaticus is a rare cause of
gastrointestinal bleeding during pregnancy and remains one of the most
challenging diagnostic and management dilemmas to physicians. Early suspicion
and serial endoscopic examination in pregnant women with abdominal pain and
gastrointestinal bleeding may result in appropriate diagnosis.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding was received on this work.
REFERENCES
1. Suter M, Doenz F, Chapuis G, Gillet M, Sandblom P. Haemorrhage into the pancreatic duct (Hemosuccus pancreaticus): recognition and management. Eur J Surg 1995; 161:887-892.
2. Etienne S, Pessaux P, Tuech JJ, Lada P, Lermite E, Brehant O, et al. Hemosuccus pancreaticus: a rare cause of gastrointestinal bleeding. Gastroenterol Clin Biol. 2005 Mar; 29(3):237-242.
3. Peroux JL, Arput JP, Saint-Paul MC, Dumas R, Hastier P, Caroli FX, et al. Wirsungorragie compliquant une pancréatite chronique associée à une tumeur neuroendocrine du pancréas. Gastroenterol Clin Biol 1994; 18: 1142-1145.
4. Kim SS, Roberts RR, Nagy KK, Joseph K, Bokhari F, An G, et al. Hemosuccus pancreaticus after penetrating trauma to the abdomen. J Trauma 2000; 49:948-950.
5. Quan WL, Chia CK, Yim HB. Safety of endoscopical procedures during pregnancy. Singapore Med J. 2006 Jun; 47(6):525-528.
6. Koizumi J, Inoue S, Yonekawa H, Kunieda T. Hemosuccus pancreaticus: diagnosis with CT and MRI and treatment with transcatheter embolization. Abdom Imaging 2002; 27: 77-81.
7. Arnaud JP, Bergamaschi R, Serra-Maudet V, Casa C. Pancreatoduodenectomy for hemosuccus pancreaticus in silent chronic pancreatitis. Arch Surg 1994; 129:333-334.
8. Lermite E, Regenet N, Tuech JJ, Pessaux P, Meurette G, Bridoux V, et al. Diagnosis and treatment of hemosuccus pancreaticus: development of endovascular management. Pancreas 2007 Mar; 34(2):229-232.