
Laparo-endoscopic Assisted Percutaneous Drainage Gastrostomy and Feeding Jejunostomy
Vishwanath Golash
doi:10.5001/omj.2010.66
From the Department of Department of Obstetrics and Gynaecology, Oman Medical College, Sohar, Sultanate of Oman.
Received: 13 Feb 2010
Accepted: 21 Apr 2010
Address correspondence and reprint request to: Vishwanath Golash, Sr. Consultant Surgeon, Head Department of Surgery, Sultan Qaboos Hospital, Oman
E-mail: golash@omantel.net.om, haritagolash@hotmail.com
Acquired tracheo-esophageal Fistula (TEF) is a rare but serious complication of prolonged endotracheal intubation. Patients of TEF are usually very critically ill and prone to repeated aspiration and pneumonia. The first stage of treatment involves the diversion of salivary and gastric contents away from the fistula site, improving the nutritional status and control of sepsis. A drainage gastrostomy and feeding jejunostomy is often required to divert the gastric contents away from the fistula and for nutrition.
There are several methods of diversion of gastric contents and for creating feeding jejunostomy including percutaneous, endoscopic, radiological, laparoscopy and laparotomy, tailored according to the clinical situation and the available expertise. In this patient, percutaneous approach alone was not possible due to past and present abdominal surgery and obesity. A combined laparoscopic and endoscopic technique was used to create a drainage gastrostomy and feeding jejunostomy. TEF was repaired three months later.
A 35 year old full term multipara female was referred from a neighboring country with a history of obstructed labor for the last three days. On examination, the patient was toxic, febrile, dyspnoic. Her abdomen was tense, tender, and had a scar from previous caesarian section and yet no fetal heart sounds were audible. The chest was full of bilateral crepitations. The initial diagnosis on admission was pre-eclampsia, intrauterine death of child, pneumonia and septicemia. An urgent U/S of the abdomen showed a full term uterus and no fetal movements. The chest X-ray and CT scan of the chest were suggestive of aspiration pneumonia.
The patient was resuscitated. The dead fetus and placenta were delivered by emergency caesarian section. Her postoperative recovery was stormy. A tracheotomy was performed to assist in the ventilator. She was weaned from parental nutrition and was fed through the nasogastric tube. Four weeks after her tracheostomy, contents of nasogastric tube feeding were seen coming through the tracheotomy tube. A tracheo-esophageal fistula was suspected and confirmed by imaging studies and endoscopy.
On Endoscopy the inflated cuff balloon of the tracheostomy tube was seen through the esophagus The TEF was of more than 2 cm in size, (Fig. 1). The case was discussed in a multidisciplinary meeting and in the view of extreme obesity with the history of past and recent surgery, percutaneous endoscopic gastrostomy (PEG) was considered unsafe.
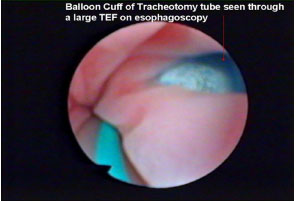
Figure 1: Endoscopic view of TEF
Among the other alternatives, the laparoscopic approach was considered safer than open approach. The procedure was explained to the patient’s relative and consent taken. A diversion laparoscopic gastrostomy and feeding jejunostomy was performed as follows:
Surgical procedure: Pneumoperitoneum was created through a 10 mm umbilical port inserted by open technique. Laparoscopy was performed in supine position using 00 laparoscope under 12 mm Hg CO2 pressure.
The greater omentum was adherent at the site of previous surgery and as well as to the anterior abdominal wall. There were other unexplained adhesions in the abdominal cavity suggestive of some inflammatory pathology in the past. Further two 5 mm ports were inserted under vision in the epigastrium and in the left midclavicular line. (Fig. 2)

Figure 2: Port position
Adhesiolysis was performed to clear the anterior aspect of stomach. A 1cm anterior gastrostomy was created with the help of ultracision in the lower third of the stomach closer to lesser gastric curvature. The stomach was held on two nylon stay sutures to help in the introduction of the gastric tube (PEG 24, Pull type, Cook Wilson medical G.I. endoscopy) and later these two stay sutures were tied subcutaneously to fix the stomach to the anterior abdominal wall. (Fig. 3)
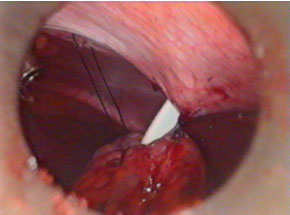
Figure 3: Nylon stay sutures on stomach
A 120 cm long size ‘8’ pediatric nasogastric tube on a stent was threaded through the gastrostomy tube, (Fig. 4). On gastroscopy, the tip of the pediatric nasogastric tube was grasped by biopsy forceps in the stomach and the gastroscope was maneuvered in the third part of duodenum.

Figure 4: Gastro-jejunostomy tube combination
The biopsy forceps was released, the nasogastric tube was further advanced in the jejunum and gastroscope was withdrawn. The position of jejunostomy tube was further confirmed by gastrograffin studies. (Fig. 5)

Figure 5: Injection jejunogram
The gastrostomy tube was used for the gastric suction and free drainage and the jejunostomy tube was used for feeding. Jejunostomy feeding was established by a pump. (Fig. 6)
The patient’s general condition slowly improved and the sepsis was controlled. Three months later, TEF was repaired through a single stage procedure with two interposition muscle pedicle flaps
and a new tracheostomy was created further down the tracheal suture line. (Figs. 7, 8, 9)

Figure 6: Jejunostomy feeding by pump
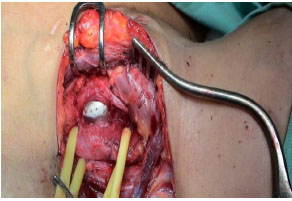
Figure 7: Large TEF

Figure 8: Repaired TEF

Post operatively, the jejunostomy feeding was continued. The gastrograffin swallow study performed a week after the repair of tracheo-esophageal fistula showed no sign of leakage at the TEF site.
Figure 9: Muscle pedicle flaps sutured over TEF repair
The patient was gradually resumed to normal oral feeding and the gastrostomy tube with the jejunostomy tube was removed after three weeks and tracheotomy closed after 1 month.
Laparoscopy combined with gastroscopy was successful in placing gastrostomy and jejunostomy tubes. There was no infection, blockage, leakage, migration of either of the tubes during their entire course of use. There was no retrograde reflux as no aspiration of jejunostomy feeding was seen coming through the gastrostomy tube. There were no complications of primary repair of the TEF. The patient was seen a year after the surgery in normal health and there was no evidence of tracheal stenosis or recurrence of TEF.
Overall, laparo-endoscopic perioperative drainage gastrostomy and tube jejunostomy is safe and feasible for long term enteral nutrition.
The percutaneous endoscopic gastrostomy (PEG) and percutaneous endoscopic jejunostomy (PEJ) are established standard procedures for long term enteral nutrition and have replaced the open techniques. The PEG is most commonly performed for enteral feeding but PEJ is preferred to avoid complications of aspiration pneumonia associated with tube gastrostomy.1,2 Both percutaneous techniques are not suitable in morbidly obese and patients with previous abdominal surgery as was seen in the studied patient. Moreover, the percutaneous technique of jejunostomy is difficult to learn and practice. When the percutaneous method is not possible, laparoscopy is an excellent alternative option for placing gastrostomy and jejunostomy tubes.
Laparoscopic methods have several advantages, for example; excellent exposure, accurate and secure placement of tubes under vision, lysis of adhesions and avoids injury to other abdominal viscera. It also presents less chances of leakage, peritonitis and displacement of the tubes.3,4 Several authors have shown the advantages of laparoscopic or laparoscopic guided gastrostomy and jejunostomy.
Zamakhshary et al. used laparoscopic approach primarily considering it is safer and easier to perform with results as good as percutaneous methods.5 Takahashi et al. preferred the lap assisted PEG as their method of choice because it allowed its safe placement.6 Duh et al. prospectively evaluated the laparoscopic jejunostomy and reported it to be safe with no serious complications.7 Nagle and Murayama in their review of various techniques have shown comparative favorable results of laparoscopic with corresponding open surgical procedures.8 Crowshaw and Nottingham indicated laparoscopic gastrostomy after failure of PEG.9 Han-Geurts et al. conducted an extensive systemic review of techniques for feeding jejunostomy and reported the advantages of minimal access surgery and its safety.10
There are several laparoscopic techniques in practice for the placement of gastrostomy and jejunostomy tubes. Normally, a feeding gastrostomy and jejunostomy is created by direct gastrostomy or enterotomy using a standard pre-packed Kits but several other alternative approaches have been described. Duh and Lawrence have described their technique of laparoscopic gastrostomy and jejunostomy using T-fasteners as retractors and anchors.11,12 While Allen et al. published a simple cost effective totally laparoscopic technique of placing a ‘T’ tube for feeding jejunostomy.13 Antonoff et al. have used a modified approach for Lap PEG to avoid suture associated complications.14
On the other hand, Sangster and Swanstrom in their method used a red rubber catheter for feeding jejunostomy and a balloon catheter for decompression of the stomach, while Gui et al. used a suprapubic catheter set sheath for creating jejunostomy.15,16 Denzer et al. developed a mini-laparoscopic assisted technique of tube placement as an alternative to when PEG is not possible.17
In the studied patient, the placement of jejunostomy tube was improvised (a fine pediatric nasogastric tube) percutaneously through the gastrostomy tube and maneuvered it passed the ligament Treitz in the jejunum by the help of gastroscope. This avoided the need for a separate enterotomy and its associated complications.
In this patient of TEF, the primary function of PEG was not of enteral nutrition but to use it for aspiration and continuous drainage of gastric contents to prevent aspiration pneumonia.
The laparoscopy was successfully used to visually guide the percutaneous gastrostomy tube and gastroscopy to manoeuvre the jejunostomy tube in the jejunum.
The placing the PEG and jejunostomy tube by laparo-endoscopy method had a dual advantage of PEG and as an open procedure. The laparoscopic gastrostomy and jejunostomy is superior in terms of complications and outcome. The visible control makes it simple and safe.
ACKNOWLEDGEMENTS
The author reported no conflict of interest and no funding was received on this work.
-
Hassett JM, Sunby C, Flint LM. No elimination of aspiration pneumonia in neurologically disabled patients with feeding gastrostomy. Surg Gynecol Obstet. 1988 Nov;167(5):383-8.
-
Jarnagin WR, Duh QY, Mulvihill SJ, Ridge JA, Schrock TR, Way LW. The efficacy and limitations of percutaneous endoscopic gastrostomy. Arch Surg. 1992;127 (3):261-264.
-
Edelman DS. Laparoendoscopic approaches to enteral access. Semin Laparosc Surg. 2001 Sep;8(3):195-201.
-
Yu SC, Petty JK, Bensard DD, Partrick DA, Bruny JL, Hendrickson RJ. Laparoscopic-assisted percutaneous endoscopic gastrostomy in children and adolescents. JSLS. 2005 Jul-Sep;9(3):302-4.
-
Zamakhshary M, Jamal M, Blair GK, Murphy JJ, Webber EM, Skarsgard ED. Laparoscopic vs percutaneous endoscopic gastrostomy tube insertion: a new pediatric gold standard? J Pediatr Surg. 2005 May; 40(5):859-62.
-
Takahashi T, Okazaki T, Kato Y, Watayo H, Lane GJ, Kobayashi H, et al. Laparoscopy-assisted Percutaneous Endoscopic Gastrostomy. Asian J Surg 2008 Oct; 31(4):204-6.
-
Duh QY, Senokozlieff-Englehart AL, Siperstein AE, Pearl J, Grant JP, Twomey PL, et al. Prospective evaluation of the safety and efficacy of laparoscopic jejunostomy. West Med 1995; 162 (2):117-122.
-
Nagle AP, Murayama KM. Laparoscopic gastrostomy and jejunostomy. J Long Term Eff Med Implants. 2004; 14(1):1-11.
-
Croshaw RL, Nottingham JM. Laparoscopic-assisted percutaneous endoscopic gastrostomy: its role in providing enteric access when percutaneous endoscopic gastrostomy is not possible. Am Surg 2006 Dec; 72(12):1222-4.
-
Han-Geurts IJM, Lim A, Stijnen T, Bonjer HJ. Laparoscopic feeding jejunostomy A systematic review Surg Endosc 2005; 19 (7): 951–957.
-
Duh QY, Way LW. Laparoscopic gastrostomy using T-fasteners as retractors and anchors. Surg Endosc 1993: 7 (1):60-63.
-
Duh QY, Way LW. Laparoscopic jejunostomy using T-fasteners as retractors and anchors. Arch Surg 1993; 128 (1):105-108.
-
Allen JW, Ali A, Wo J, Bumpous JM, Cacchione RN. Totally laparoscopic feeding jejunostomy. Surg Endosc 2002; 16 (12): 1802–1805.
-
Antonoff MB, Hess DJ, Saltzman DA, Acton RD. Modified approach to laparoscopic gastrostomy tube placement minimizes complications Pediatric surgery international. 2009 Apr; 25(4):349-53 .
-
Sangster W, Swanstrom L. Laparoscopic-guided feeding jejunostomy Surg Endosc. 1993 Jul-Aug;7(4):308-10.
-
Gui GPH, Fiennes AGTW, Cheruvu CVN. Intracorporeal laparoscopic-guided feeding jejunostomy Ann R Coll Surg Engl 1997; 79 (6): 462-463.
-
Denzer U, Mergener K, Kanzler S, Kiesslich R, Helmreich-Becker I, Galle PR, et al. Mini-laparoscopically guided percutaneous gastrostomy and jejunostomy. Gastrointest Endosc. 2003; 58(3):434-8.
How to cite this article
Golash V. Laparo-endoscopic Assisted Percutaneous Drainage Gastrostomy and Feeding Jejunostomy. OMJ 2010 July; 25(3):234-237.
How to cite this URL
Golash V. Laparo-endoscopic Assisted Percutaneous Drainage Gastrostomy and Feeding Jejunostomy. OMJ [Online] 2010 July; 25(3):234-237. Available at http://www.omjournal.org/BriefCommunication/FullText/201007/FT_Laparo-endoscopicAssistedPercutaneous.html