
Looser’s Zone
Feroze Ahmad, Bashir Shah, Ghulam Nabi, Fayaz Sofi
Ahmad F, et al. OMJ. 25, 141 (2010); doi:10.5001/omj.2010.38
From the Department of General Medicine, SKIMS Soura, India,
Received: 05 Dec 2009
Accepted: 28 Jan 2010
Address correspondence and reprint request to: Dr. Feroze Ahmad Department of General Medicine, SKIMS Soura, India
Email: drferozeahmad@rediffmail.com
Ahmad F, et al. OMJ. 25, 141 (2010); doi:10.5001/omj.2010.38
Osteomalacia is usually neglected when compared with other metabolic bone diseases and may present with a variety of clinical and radiographic manifestations mimicking other musculoskeletal disorders. It is a known cause of persistent, nonspecific musculoskeletal pain.
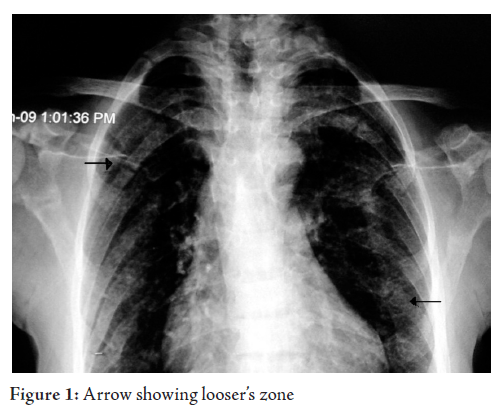
A 35 year old female was admitted with generalized aches and pains for the last two years. She was of thin stature with a BMI of 18 kg/m2, indicative of malnourishment. On examination, vital signs were normal. She had generalized bony tenderness, proximal muscle weakness of both lower limbs. Neurological examination was also normal. Electrolytes were normal. Serum chemistry showed calcium was 8.81 mg/dl, normal ALP and albumin. The rest of the investigations were within normal limits. Chest X ray showed normal parenchyma with looser’s zones. (Fig. 1, 2)
Osteomalacia is commonly neglected because it presents with a variety of clinical and radiographic manifestations mimicking other musculoskeletal disorders. 1 It is a knowIt is a known cause of persistent, nonspecific musculoskeletal pain. Patients with osteomalacia can present with diffuse pain that may be misdiagnosed as fibromyalgia. Patients proven to have osteomalacia on bone biopsy have pseudo fractures on Radionuclide bone scan present with regional or widespread pain.1
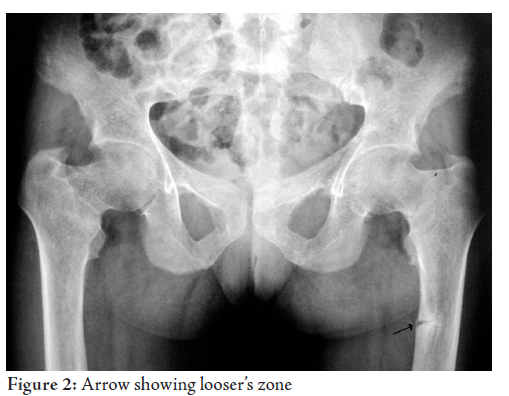
Mechanical stress of the main blood vessels overlying the uncalcified cortex of osteomalacic bones is regarded as the factor determining the location of the symmetrical pseudo fractures.2,3 The “pseudo-fractures” typically show as transverse zones of rarefaction, varying in width from 1 mm to 1 cm. They are multiple and generally symmetrical in distribution, and often occur in apparently normal bone. Their distribution is mainly ischio-pubis, ilio-pubis, femur, tibia, radius, fibula, or at the iliac bone. 4 Other common sites are the lower ribs and the infraglenoid region of the scapula.
This patient responded satisfactorily to 60000 units of vitThis patient responded satisfactorily to 60000 units of vitamin D per day for 7 days followed by 60000 units monthly.
REFERENCES-
Reginato AJ, Falasca GF, Pappu R, McKnight B, Agha A. Musculoskeletal manifestations of osteomalacia: report of 26 cases and literature review. Semin Arthritis Rheum 1999; 28:287-304. M, Blunt JW Jr, A Factor Determining the Location of Pseudofractures in Osteomalacia. J. Clin. Invest 1949; 28:521.
-
Steinback H. Kolb FO, Gilfillan R. A Mechanism of the Production of Pseudofractures in Osteomalacia. Radiology 62: 388, 1954.
-
Stanley Nowell, Evans PRC, Kurrein F. Multiple Spontaneous Pseudofractures of bone (MILKMAN?S SYNDROME). British Medical Journal 1951; 14:91.