
Correlation of Early Neonatal Mortality and Technical Efficiency of Regional Maternal and Child Health Services in Oman
Rajeev Aravindhakshan, Jayalekshmi BR, Rekha Sukumar
Aravindhakshan R,et al. OMJ. 25, 53-54 (2010); doi:10.5001/omj.2010.15
From the Department of Epidemiology and Public Health
Received: 27 Nov 2009
Accepted: 16 Dec 2009
Address correspondence and reprint requests to: Dr. Rajeev Aravindhakshan, Department of Epidemiology and Public Health,
Oman Medical College, Sohar, North Al Batinah, Sultanate of Oman
E-mail: rajeevtka@gmail.com
Health sector reforms are always linked to financial restraints. The relative low spending on healthcare by the majority of developing countries makes it even more crucial to plan the deployment of health services optimally. Many countries in the world have taken recourse to analyzing efficiency of the decision making units (DMU) in terms of inputs and outputs. A study from Ghana using this approach found 65% of the sampled health centres (HC) to be deficient in terms of services delivered in maternal and child health domains based on inputs such as number of staff, number of beds and the financial outlay.1 The method used was Data Envelopment Analysis (DEA) which gave a relative measure of efficiency.
DEA estimates how well a DMU is functioning compared to its peers. It is constructed non-parametrically using linear programming techniques and can analyze several outputs simultaneously. The technical efficiency (TE) of a DMU refers to the ability to minimize the use of inputs in reaching the given outputs or the ability to obtain the maximum output from a given set of inputs. A constant return to scale (CRS) model is applicable when all the DMUs are functioning at an optimal scale. On the other hand, a variable return to scale (VRS) model can be employed as an extension to CRS model so as not to be affected by the scale efficiency.2
The model used in the paper from Ghana was input-oriented and instead of going for a constant return to scale (CRS) model, the study used a variable return to scale (VRS) model. The scale efficiency was derived by finding the ratio of CRS efficiency score to VRS efficiency score. Pure technical efficiency and scale efficiency was proposed as an aid to find the potential of increasing the total outputs for the existing capacity/size of the DMU. The study concluded that the centres (DMU/HC) were using more inputs than needed to produce the current outputs. Hence a cost minimization objective was put forth which aimed at input savings.
In the year 2000, a DEA approach was applied to 20 hospitals in Oman.3 Four outputs representing out-patient visits, in-patient services and surgical operations, and three inputs representing the number of beds and manpower were used in the analysis. The study found 10 of those hospitals to be inefficient. Considering mortality and burden of disease as a basis for planning may not prove entirely economical. For example, there was no data on infrastructure and expenditure in the analysis of mortality of newborns which was undertaken in the Sultanate of Oman in 1999.4 On the other extreme, a pure economic model can be deleterious in a field like health sciences.
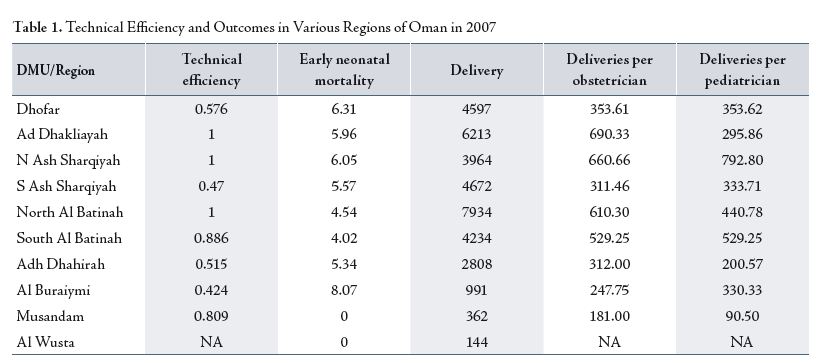
The author applied models which are suitable for a profit making organization, to a service based domain like health services. Moreover, such analyses in the past also have not considered the effect of maximizing outputs per unit input on direct outcomes of importance such as mortality. What is the alternative then for a health service specific efficiency analysis? To find an answer, a DEA analysis of MCH situation in Sultanate of Oman based on data from MOH (2007) with regions of the country as DMUs was undertaken.5 Efficiency was derived from CRS model only. The technical efficiency calculated from the analysis was correlated with the early neonatal mortality from these regions.
The regions performing most ideally (TE of 1) were having 610 to 690 deliveries per obstetrician per year.(Table 1)
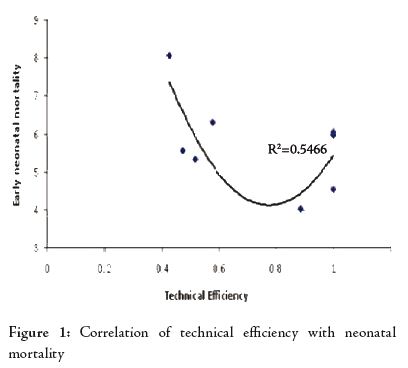
Technical efficiency also correlated well with the early neonatal mortality (ENMR) to some extent. However, the results showed that the early neonatal mortality reached the lowest value of about 4 per 1000 live births (LB) at a relative TE of 0.8 (500 deliveries per obstetrician per year), (Fig. 1). Beyond that, even though economically speaking, the regions were maximizing outputs at given input levels, the early neonatal mortality climbed up to about 4.5 to 6 per 1000 LB, irrespective of the pediatrician to delivery ratio. Obviously, there is a limit to which the system can stretch itself. Synthesis of analysis results concludes that an increase in the number of outpatient consultations and number of deliveries etc. per obstetrician beyond a point will have a negative impact on the neonatal health outcomes even at an impressive input-output ratio.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding has been received on this work.
-
Osei D, d’Almeida S, George MO, Kirigia JM, Mensah AO, Kainyu LH. Technical efficiency of public district hospitals and health centres in Ghana: a pilot study. Cost Effectiveness and Resource Allocation 2005;3. Available at http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1253524. Accessed 26-Dec-09.
-
Ramanathan TV, Chandra KS, Thupeng WM. A comparison of the technical efficiencies of health districts and hospitals in Botswana. Development Southern Africa 2003;20;307-321.
-
Ramakrishnan R. Operations assessment of hospitals in the Sultanate of Oman. International Journal of Operations & Production Management 2005; 25:39-54.
-
Ohlsson A. Report on perinatal and neonatal infant mortality in Sultanate of Oman. Ministry of Health and UNICEF; 1999;12.
-
Ministry of Health, Oman, Annual Health Report 2007, Directorate General of Planning, Department of Information and Planning, 2008.